Air-liquid interface (ALI) culture is a cell culture method in which the apical surface of airway epithelial cells is exposed to air while the basolateral surface remains in contact with culture medium. This setup supports epithelial polarization and differentiation, allowing researchers to establish human airway models with features such as cilia, mucus production, tight junctions, and epithelial barrier function.1,2
We rarely think about breathing. At rest, however, we inhale and exhale several liters of air every minute. This air contains the oxygen we need, but it can also introduce dust, pollutants, and potentially harmful pathogens into the respiratory tract.
The epithelial cells lining our airways form an important protective barrier. They help capture and remove inhaled agents before they can damage the underlying tissue. In respiratory conditions such as asthma and chronic obstructive pulmonary disease (COPD), these defense mechanisms can become impaired.3
To investigate what happens inside the airways, researchers need in vitro models that reproduce relevant features of the respiratory epithelium. Air-liquid interface (ALI) cultures provide a human-relevant system for studying airway physiology and disease, epithelial interactions with respiratory pathogens or pollutants, and responses to aerosolized drugs.
ALI systems can also contribute to the Replace, Reduce, and Refine principles, commonly known as the 3Rs, by supporting research questions that can be investigated using human airway epithelial models. However, like every in vitro system, ALI cultures require appropriate validation and controlled culture conditions to generate interpretable and reproducible results.2,4
Why is the human airway difficult to model in vitro?
The respiratory epithelium contains several specialized cell types, including basal cells, goblet cells, and ciliated epithelial cells. This cellular diversity reflects the different functions that the airway lining must perform.5
Goblet cells and seromucous glands produce mucus, which forms a protective layer and captures inhaled microorganisms and particles. Ciliated cells then move this material toward the throat through mucociliary clearance. Airway epithelial cells also produce cytokines and participate in innate and adaptive immune responses.3,6
Reproducing these functions in vitro is challenging. Conventional two-dimensional cultures often lose tissue-specific architecture and cellular differentiation. Primary bronchial epithelial cells may lose their ability to form cilia or produce mucus, while the barrier properties of the epithelium can also become altered.7
Airway-derived cell lines are useful for many applications, but some are cancer-derived or immortalized and may not fully represent the behavior of normal primary airway epithelial cells. Primary human airway epithelial cultures have therefore become increasingly important for studying differentiated respiratory tissue. Culture conditions used during initial expansion can also influence whether primary normal human bronchial epithelial cells retain the characteristics required for subsequent three-dimensional differentiation.8
ALI culture helps overcome some of the limitations of submerged monolayers. Under suitable conditions, the cells can develop a pseudostratified structure, undergo mucociliary differentiation, produce mucins, and form tight junctions.2
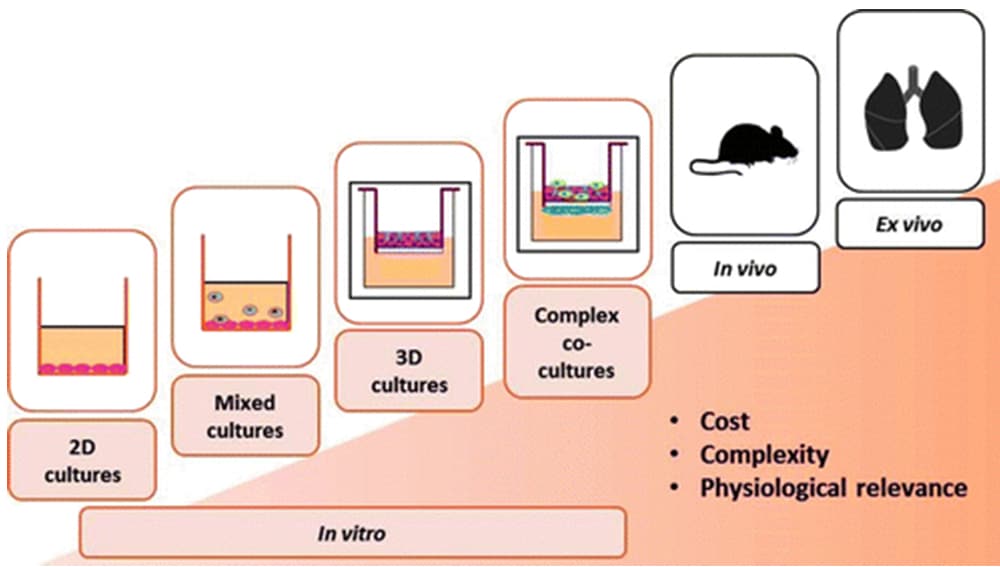
Figure 1: Different levels of complexity in respiratory research models. In vitro systems range from two-dimensional cultures to mixed cultures, three-dimensional cultures, and complex co-cultures. Increasing model complexity may improve physiological relevance, but it can also increase cost and experimental requirements.
What is air-liquid interface culture?
In an ALI culture, airway epithelial cells are grown on a permeable membrane that separates an apical and a basolateral compartment. During the differentiation phase, the apical surface is exposed to air while the basolateral surface continues to receive nutrients from the culture medium.1,2
This configuration reflects an important feature of the respiratory tract. In vivo, the apical surface of airway epithelial cells faces inhaled air, while nutrients are supplied from the underlying tissue.
Exposure to these different environments supports basoapical polarity and epithelial differentiation. Under appropriate culture conditions, the cells can form a pseudostratified epithelium with ciliated and mucus-producing cells, as well as tight junctions that contribute to barrier function.1,2
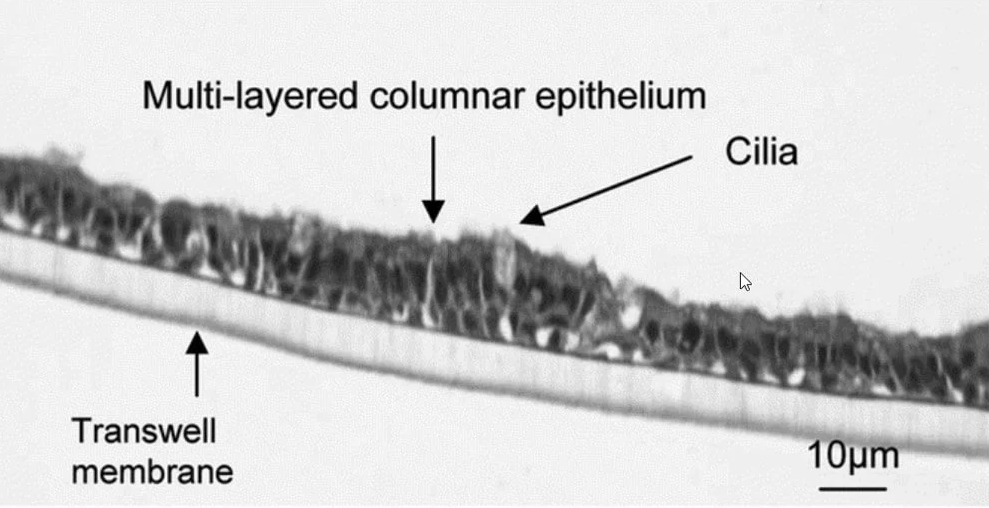
Figure 2: Differentiated human bronchial epithelial cells cultured at the air-liquid interface. The image shows a multilayered columnar epithelium with apical cilia growing on a permeable Transwell membrane.
How does air-liquid interface culture work?
An airway ALI workflow generally includes an initial expansion phase, transfer to a permeable insert, submerged culture, and differentiation after air-lifting.1
- Cell expansion: Primary airway epithelial cells are first expanded in conventional culture vessels. In the PromoCell workflow, cells are passaged once they reach approximately 70–80% confluence.
- Transfer to an insert: The expanded cells are seeded onto a porous membrane, commonly coated with an extracellular matrix component such as collagen.
- Submerged culture: Culture medium is initially present in both the apical and basolateral compartments. The cells proliferate until they form a confluent epithelial layer.
- Air-lifting: Once the layer is confluent, the apical medium is removed. Nutrients are then supplied only from the basolateral compartment, while the apical side is exposed to air.
- Differentiation: Air exposure promotes polarization and differentiation. The cells can develop cilia, produce mucus, and establish a functional epithelial barrier.
Exact culture times and handling steps depend on the selected cell type, donor, medium, insert, and protocol. In the PromoCell workflow, the differentiation phase continues for at least 14 days after air-lifting.
For detailed culture instructions, see the application note Air-Liquid Interface Culture System for Standardized Respiratory Research.
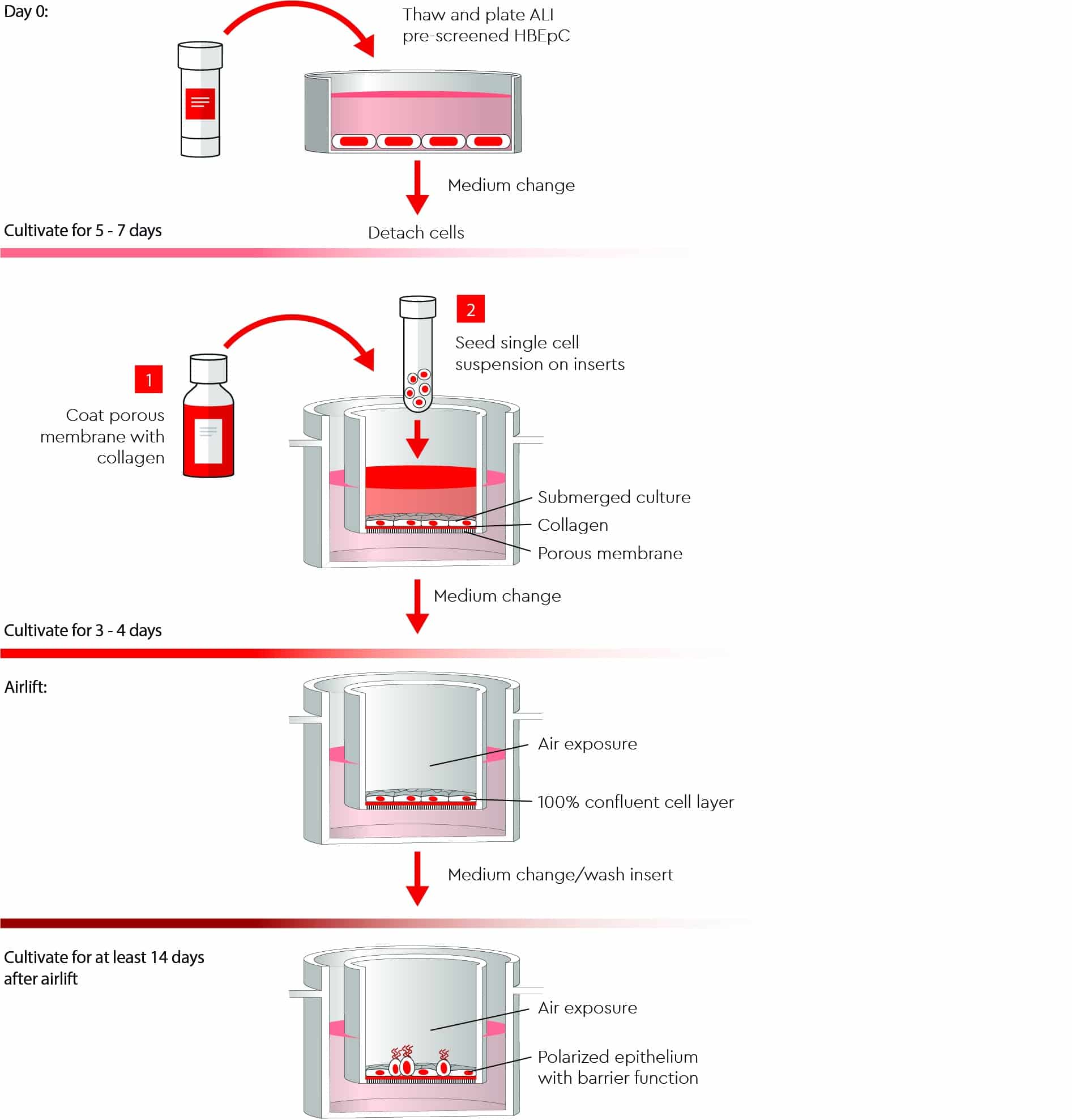
Figure 3: Main stages of an airway epithelial ALI workflow. Primary bronchial epithelial cells are expanded in two-dimensional culture, seeded onto collagen-coated permeable inserts, maintained under submerged conditions, and then air-lifted. The post-airlift phase supports epithelial polarization and barrier formation.
How is epithelial barrier integrity assessed?
Transepithelial electrical resistance (TEER) is a non-destructive measurement commonly used to assess epithelial barrier integrity. It measures the electrical resistance across the cell layer and can indicate the formation and maintenance of tight junctions.9
During the measurement, electrodes are positioned on either side of the epithelial layer and electrical resistance is recorded. Because the procedure does not destroy the culture, TEER can be measured repeatedly to monitor barrier development over time or following experimental exposure.
Earlier in vivo studies also measured transepithelial electric potential differences across the human tracheal and bronchial epithelium, helping to establish airway electrophysiology as a functional epithelial readout.10
TEER values should be interpreted in the context of the cell source, donor, insert, culture conditions, and measurement system. A single threshold should not be treated as a universal definition of a successful ALI model. Where possible, TEER should be considered together with other readouts, such as morphology, permeability, viability, tight-junction markers, cilia formation, or mucus production.9
Why are standardization and validation important in ALI culture?
ALI cultures can vary between laboratories because researchers may use different cells, donors, passages, media, inserts, coatings, seeding densities, and air-lifting schedules. These differences can make it difficult to compare results between studies.2,4
The issue is particularly important because ALI experiments commonly run for several weeks. Incomplete attachment, poor differentiation, or weak barrier formation may only become apparent after considerable time and material have already been invested.
Standardization does not mean that every laboratory must use an identical protocol. It means that the relevant culture parameters are documented, controlled, and validated for the intended research question.2,4
| Factor | Why it can affect the model | What researchers should document or control |
|---|---|---|
| Cell and donor source | Donor characteristics can influence proliferation, differentiation, and barrier formation | Tissue source, donor status, disease information, medication history where available |
| Passage and confluence | Over-confluence or extensive passaging may alter proliferation and differentiation | Passage number and confluence at passaging, seeding, and air-lifting |
| Insert and coating | Membrane properties and coating can affect attachment and barrier development | Insert material, pore size, surface area, and coating method |
| Seeding density | Uneven or insufficient seeding may delay formation of a confluent layer | Living cells seeded per cm2 and cell distribution |
| Culture medium | Medium composition affects expansion, differentiation, and barrier stability | Medium used during each phase, supplements, and lot information |
| Air-lifting and feeding schedule | Timing and handling influence differentiation | Confluence at air-lifting, medium-change schedule, and apical washing |
| Quality-control readouts | Different endpoints may capture different features of the model | TEER, morphology, viability, mucus, cilia, permeability, and marker expression |
Table 1: Factors that can influence ALI culture performance
How do donor variability and cell selection affect ALI culture?
Variation between primary-cell donors is expected. Donor characteristics, disease status, and previous medication may influence epithelial proliferation, differentiation, or barrier formation.
This biological variability can be valuable when the objective is to compare different donors or disease states. However, it may complicate studies that require a stable reference culture or positive control.
Human Bronchial Epithelial Cells that have been pre-screened for ALI culture have been evaluated for specified barrier-forming performance under defined conditions. Pre-screening can reduce the risk of selecting a donor lot with unsuitable performance for the planned workflow, but it does not eliminate biological variability or guarantee identical results in every laboratory.
Human leukocyte antigen (HLA) typing may be relevant where antigen presentation, immune recognition, or disease-associated HLA variation forms part of the research question. Bronchial epithelial cells from patients with asthma have been reported to display altered expression of functional HLA-G isoforms.11 HLA typing is not, however, a general requirement for every airway ALI study.
Why does ALI medium composition matter?
Culture medium can influence epithelial-cell expansion, differentiation, and barrier development. Researchers should distinguish between the medium used during the initial expansion phase and the medium used after air-lifting to support differentiation.2,4
Serum- and bovine pituitary extract (BPE)-free formulations can reduce variability associated with incompletely characterized supplements. They do not, however, eliminate variability arising from donors, handling, inserts, or other protocol parameters.
For a serum- and BPE-free workflow, Airway Epithelial Cell Growth Medium 2 can be used for the expansion of epithelial cells from large air passages and combined with Air-Liquid Interface Medium during the differentiation phase.
To explore this variable in more detail, read our technical resources on how Air-Liquid Interface media compositions can influence epithelial barrier integrity.
What are ALI cultures used for in respiratory research?
ALI systems are used to investigate processes that depend on differentiated airway epithelium, epithelial barrier function, or exposure at the air-facing surface. Applications include disease modeling, infection research, inhaled-drug studies, and toxicology.2,3
You can explore additional cell types and resources on our respiratory research overview page.
Respiratory disease models
Airway epithelial cells from healthy donors or donors with respiratory conditions can be cultured at the air-liquid interface to investigate disease-associated changes in epithelial function.
ALI cultures have been used in research into asthma, chronic obstructive pulmonary disease, cystic fibrosis, pneumonia, and other respiratory conditions. Depending on the model, researchers can evaluate endpoints such as barrier integrity, mucus production, ciliary function, cytokine release, epithelial repair, or gene expression.3
Inhalation and drug-delivery studies
ALI systems are particularly relevant when studying substances delivered to the air-facing surface of the respiratory epithelium.
In submerged culture, a compound added to the medium may contact the entire cell surface. In an ALI model, aerosols or droplets can be applied to the apical side, more closely reflecting the route by which inhaled drugs reach airway epithelial cells.
Researchers can use these systems to investigate epithelial uptake, barrier transport, biological responses, and local toxicity. The deposited dose and exposure conditions still need to be characterized carefully.12
Respiratory infection research
Viruses and bacteria can be applied to the apical surface of differentiated airway epithelial cultures. This enables researchers to investigate pathogen entry, replication, epithelial damage, and host responses in a human airway model.
ALI cultures have been used to study respiratory pathogens including influenza viruses, respiratory syncytial virus, and SARS-CoV-2. Variation in host immune responses is also an important consideration in COVID-19, where differences in disease severity cannot be explained by viral exposure alone.13
For example, Mulay et al. differentiated primary human proximal airway epithelial cells at the air-liquid interface and used the resulting mucociliary cultures to investigate SARS-CoV-2 infection, epithelial host responses, and candidate drug effects.14
Toxicology and air-pollution research
ALI exposure systems allow researchers to study epithelial responses to particles, gases, tobacco smoke, air pollutants, and other inhaled substances.
Because the material can be applied directly to the air-facing surface, researchers can investigate effects on barrier integrity, viability, inflammatory signaling, mucus production, and ciliary function. ALI models can therefore complement conventional in vitro and in vivo approaches in respiratory toxicology.2,15
No single ALI model can reproduce the complete respiratory system. Standard epithelial models generally lack the full immune, vascular, stromal, and mechanical environment of the lung unless these components are added through co-culture or more complex systems.2,15
ALI culture provides a closer look at airway epithelial function
Air-liquid interface culture enables primary human airway epithelial cells to develop structural and functional properties that are difficult to maintain in conventional submerged cultures. These models can support research into airway physiology, respiratory disease, infection, inhaled substances, and epithelial barrier function.
Reliable results depend on the complete experimental system. Cell source, donor, passage, insert, medium, air-lifting, and quality-control readouts should therefore be selected and documented according to the research question.
At PromoCell, we offer high-quality primary human airway epithelial cells and specialized media for different stages of airway culture, from initial cell expansion to differentiation at the air-liquid interface.
Frequently asked questions about air-liquid interface culture
References
Expand
- Chen S, Schoen J. Air-liquid interface cell culture: From airway epithelium to the female reproductive tract. Reprod Domest Anim. 2019;54(Suppl 3):38–45. doi:10.1111/rda.13481
- Lacroix G, Koch W, Ritter D, et al. Air–Liquid Interface In Vitro Models for Respiratory Toxicology Research: Consensus Workshop and Recommendations. Appl In Vitro Toxicol. 2018;4(2):91–106. doi:10.1089/aivt.2017.0034
- Mertens TCJ, Karmouty-Quintana H, Taube C, Hiemstra PS. Use of airway epithelial cell culture to unravel the pathogenesis and study treatment in obstructive airway diseases. Pulm Pharmacol Ther. 2017;45:101–113. doi:10.1016/j.pupt.2017.05.008
- Zscheppang K, Berg J, Hedtrich S, et al. Human Pulmonary 3D Models For Translational Research. Biotechnol J. 2018;13(1):1700341. doi:10.1002/biot.201700341
- Miller AJ, Spence JR. In Vitro Models to Study Human Lung Development, Disease and Homeostasis. Physiology (Bethesda). 2017;32(3):246–260. doi:10.1152/physiol.00041.2016
- Rogers DF. Physiology of Airway Mucus Secretion and Pathophysiology of Hypersecretion. Respir Care. 2007;52(9):1134–1146; discussion 1146–1149. doi:10.4187/respcare.07521134
- Ramirez RD, Sheridan S, Girard L, et al. Immortalization of Human Bronchial Epithelial Cells in the Absence of Viral Oncoproteins. Cancer Res. 2004;64(24):9027–9034. doi:10.1158/0008-5472.CAN-04-3703
- Rayner RE, Makena P, Prasad GL, Cormet-Boyaka E. Optimization of Normal Human Bronchial Epithelial (NHBE) Cell 3D Cultures for in vitro Lung Model Studies. Sci Rep. 2019;9:500. doi:10.1038/s41598-018-36735-z
- Papazian D, Würtzen PA, Hansen SWK. Polarized Airway Epithelial Models for Immunological Co-Culture Studies. Int Arch Allergy Immunol. 2016;170(1):1–21. doi:10.1159/000445833
- Knowles MR, Buntin WH, Bromberg PA, Gatzy JT, Boucher RC. Measurements of Transepithelial Electric Potential Differences in the Trachea and Bronchi of Human Subjects In Vivo. Am Rev Respir Dis. 1982;126(1):108–112.
- Carlini F, Picard C, Garulli C, et al. Bronchial Epithelial Cells from Asthmatic Patients Display Less Functional HLA-G Isoform Expression. Front Immunol. 2017;8:6. doi:10.3389/fimmu.2017.00006
- Lenz AG, Stoeger T, Cei D, et al. Efficient Bioactive Delivery of Aerosolized Drugs to Human Pulmonary Epithelial Cells Cultured in Air–Liquid Interface Conditions. Am J Respir Cell Mol Biol. 2014;51(4):526–535. doi:10.1165/rcmb.2013-0479OC
- Shi Y, Wang Y, Shao C, et al. COVID-19 infection: the perspectives on immune responses. Cell Death Differ. 2020;27(5):1451–1454. doi:10.1038/s41418-020-0530-3
- Mulay A, Konda B, Garcia G Jr, et al. SARS-CoV-2 infection of primary human lung epithelium for COVID-19 modeling and drug discovery. Cell Rep. 2021;35(5):109055. doi:10.1016/j.celrep.2021.109055
- Upadhyay S, Palmberg L. Air-Liquid Interface: Relevant In Vitro Models for Investigating Air Pollutant-Induced Pulmonary Toxicity. Toxicol Sci. 2018;164(1):21–30. doi:10.1093/toxsci/kfy053
Serum-free cell culture medium for epithelial cells from large air passages.
Primary Human Bronchial Epithelial Cells isolated from the surface epithelium of human bronchi.
Serum-free and BPE-free cell culture medium for an optimal and standardized culture of human bronchial epithelial cells at the air-liquid interface (ALI).
Related products


